Polycystic ovary (PCO) correlates with overweight / obesity in nearly 50% of cases. But is it the PCO that increases body weight or vice versa?
What is the polycystic ovary?
Definition, causes and symptoms
Polycystic ovary (PCO) is a syndrome that affects only the female sex; the name derives from the presence of numerous (and more or less large) ovarian cysts.
The main symptoms of polycystic ovary are: amenorrhea / irregular cycles, hirsutism and obesity. The symptoms are due to the increase in androgen hormones and the absence of ovulation. For this reason, problems of acne, androgenetic alopecia and infertility are also common, while the distribution of body fat takes on typically male characteristics, with preferential accumulation in the trunk and abdomen area.
The polycystic ovary can be of a metabolic or hereditary nature but the prevalence of one or the other factor, often overlapping, is not yet well known. Rarely, PCO symptoms are associated with Cushing's syndrome, adrenal hyperplasia, or ovarian and / or adrenal tumors.
The polycystic ovary is due to the immoderate increase in the synthesis of male sex hormones by the ovary; this occurs mainly under the stimulus of increased levels of LH secreted by the pituitary and circulating in the blood. Sometimes, there is also an increase in prolactin, while the levels of FSH are - in proportion - always lower than the norm; these endocrine alterations prevent the follicles from maturing and this gives rise to small ovarian cysts. It is also important to underline that, through a feed-back system, the alteration of the balance between circulating steroid sex hormones contributes to foment the dysfunction of the pituitary gland in the release of LH (perpetual cycle of the polycystic ovary).
Regarding the correlation between overweight and polycystic ovary, below we will see in more detail what are the mechanisms involved in weight gain (metabolic compromises), what preventive or curative actions to take, and how to lose weight while suffering from polycystic ovary.
Correlation with overweight / obesity
Among the metabolic factors related to polycystic ovary, insulin resistance is highlighted, that is the reduced uptake of the hormone that leads to hyper-insulinemia.
Insulin is a fattening hormone, as it has an indiscriminate anabolic effect, both for muscle and for adipose tissue. The increase in insulin in the blood is typically linked to an over-production of the hormone by the pancreas (stimulated by food), associated with a reduced ability to uptake it by the receptors present in different tissue cells (eg. skeletal muscle); the latter defect has a strong genetic component.
The ovary can also be affected by insulin resistance and this would lead to an increase in the secretion of steroid sex hormones.
We recall that ovarian hypersecretion mainly concerns the release of estrogens, and not of androgens; however, these steroid sex hormones undergo conversion to androgens due to processing by fat cells (subcutaneous fat - see aromatase enzyme).
To complete the cycle: the increase in androgen hormones causes the alteration of LH levels and the consequent triggering of the perpetual mechanism typical of the polycystic ovary.
In many cases, the resolution of insulin resistance and the decrease in adipose fat lead to the improvement of fertility and the reduction of complications induced by the polycystic ovary.
To conclude, insulin resistance increases the risk of developing polycystic ovary regardless of hereditary predisposition for endocrine ovarian dysfunction. At the same time, obesity (induced or triggering insulin resistance) increases the transformation of sex hormones, worsening the overall clinical picture. Therefore, in order to prevent / treat overweight and insulin resistance, therefore the hyperproduction of estrogen and the related conversion of androgens, it is necessary:
- maintain a normal weight or undertake dietary therapy (polycystic ovary diet)
- maintain or initiate a course of motor therapy
- evaluate the relevance of other therapeutic means (drugs and surgery).
Prevention and treatment
The first preventive action to be taken for the polycystic ovary is to maintain a normal weight in childhood and then in adolescence (therefore throughout the pubertal period). This can be achieved by:
- Education (not just food) and teaching
- Promotion of physical and motor / sports activity
- Guarantee of a balanced diet, with few junk-food foods and care of home nutrition (it is advisable to encourage the consumption of the meal in the family).
Not least, the medical evaluation for polycystic ovary familiarity in the immediate period following the menarche (especially in the case of evident clinical symptoms and signs).
As for the treatment of polycystic ovary complications, in case of insulin resistance, it is FUNDAMENTAL to apply a diet with a low index and glycemic load; moreover, in the event that there is also a picture of overweight / obesity, this dietary scheme must also pursue a real weight loss by reducing calories (low-calorie diet) and combining it with a desirable physical activity program.
More generally, the polycystic ovary can be prevented and treated by reducing androgens; this can be achieved
- through drug administration (contraceptive pill, androgen receptor blocker, favoring the secretion of FSH)
- surgically (tissue resection of the ovary or - rarely - liposuction)
- for slimming.
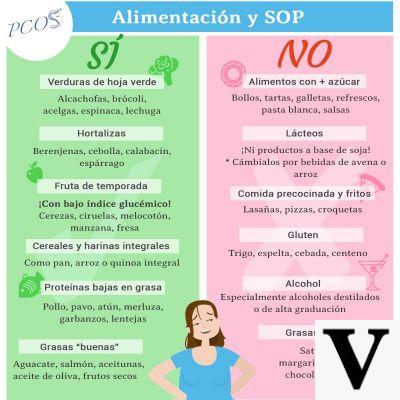
Diet
The diet for the polycystic ovary, in the presence of insulin resistance and overweight / obesity, must follow some fundamental principles. Among these, the main ones are:
- Energy intake suitable for the moderation of body fat. It is a low-calorie diet aimed at slimming, that is, the rebalancing between lean mass (FFM) and fat mass (FM). The total calories should be around 70% of those needed to maintain weight, resulting in an approximate decrease of between 2,5 and 3,5kg per month. Better not to exceed with the energy restriction to avoid nutritional depletion or unnecessary psychological stress.
- Nutritional balance through correct distribution of total calories:
- 25% (adults) or 30% (growing subjects) of total lipids; the saturated ones must not exceed 10% of the TOT energy;
- proteins must be between 0,8 and 1,2g / kg of PHYSIOLOGICAL weight;
- the rest of the energy is provided by carbohydrates. We remind you NOT to exceed with the intake of simple sugars, in particular those added or contained in processed foods; better to stay in a range between 10-12% of total calories.
- Ensure a cholesterol intake NEVER exceeds 300mg / day.
- Prefer polyunsaturated fatty acids, with an adequate intake of omega-6 and omega-3, in order to improve a physical condition potentially at risk of other metabolic complications, even on an inflammatory basis.
- The fibers must be taken at LEAST in quantities of 30g / day, since in addition to preserving intestinal function, they will facilitate the moderation of the glycemic index of meals. All vitamins and minerals must be included in the recommended rations.
- The distribution of meals must include at least 5 meals a day (preferably 6), a precaution that guarantees a moderate glycemic load; for the same reason, portions must also be carefully established.
- Choice of foods with a low glycemic index and association of all major sources of carbohydrates with good amounts of dietary fiber. Better NOT to dissociate macronutrients to ensure slow nutrient absorption (further moderation of the glycemic index). Prefer sources of whole and natural carbohydrates; reduce those refined or processed.
- To facilitate the path of weight loss and restoration of insulin sensitivity, it is advisable to start a physical activity protocol characterized by: aerobic activity (fast walking, running, cycling, swimming, rowing, canoeing, etc.) for at least 4 sessions a week, and anaerobic activity (muscle strengthening) for at least 2 sessions per week (free body exercises and / or with overloads / isokinetic machines).
For more details on the structuring of the diet for polycystic ovary it is recommended to consult the article: example diet for polycystic ovary.
Other articles on 'Polycystic Ovary: Does It Make You Fat? Diet for the Polycystic Ovary '
- polycystic flow, insulin resistance and nutrition
- Polycystic ovary
- Polycystic ovary: diagnosis and therapy
- Drugs for the treatment of Polycystic Ovary Syndrome
- Example diet for the polycystic ovary