Definition and Causes
What is meant by High Blood Pressure in Pregnancy?
La blood pressure it begins to decrease progressively after the first weeks of pregnancy, stabilizing around 75 mmHg (diastolic pressure) for the rest of the first and second trimester of gestation. In the last two - three months preceding the birth, however, the blood pressure values return to pre-pregnancy levels, therefore around 85 mmHg as regards the diastolic. We talked about minimum pressure, since the drop is mainly borne by the diastolic blood pressure (PAD) and - beyond the starting values - in the first and second trimester it can be quantified in about 7-10 mmHg.
 The decrease in blood pressure during the early stages of pregnancy is essentially linked tovasodilatory effect - hypotensive of details hormones and cytokines, which is followed by an increase in the volume of circulating blood (an effect in itself hypertensive), cardiac output and glomerular filtration.
The decrease in blood pressure during the early stages of pregnancy is essentially linked tovasodilatory effect - hypotensive of details hormones and cytokines, which is followed by an increase in the volume of circulating blood (an effect in itself hypertensive), cardiac output and glomerular filtration.
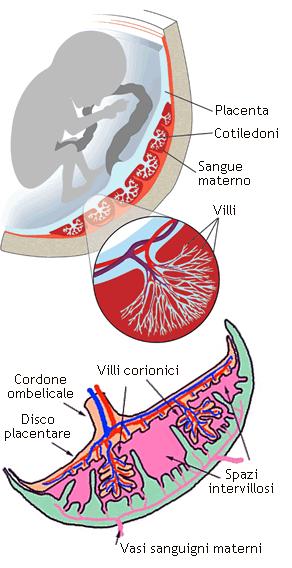
A very important organ for the success of pregnancy is the placenta, which represents the communication interface between mother and fetus. At this level, in fact, thanks to an articulated system of blood vessels and microvessels, the exchange of nutrients, waste substances and gases takes place between the blood of the two organisms, without direct contact between the two fluids. In order for all these exchanges to take place, it is necessary that a considerable amount of maternal blood reaches the placenta, with reduced speed and equally low pressure.
A very important organ for the success of pregnancy is the placenta, which represents the communication interface between mother and fetus. At this level, in fact, thanks to an articulated system of blood vessels and microvessels, the exchange of nutrients, waste substances and gases takes place between the blood of the two organisms, without direct contact between the two fluids. In order for all these exchanges to take place, it is necessary that a considerable amount of maternal blood reaches the placenta, with reduced speed and equally low pressure.
When the formation of the placenta it is not complete o is defective, the final product does not work as it should: its resistances, not sufficiently low, induce an increase in pressure upstream, that is, in the maternal organism. Unfortunately, during pregnancy, high blood pressure is dangerous for maternal and fetal health, so much so that in extreme cases it can endanger the very life of both organisms. This form of hypertension, which affects about 6-8% of pregnant women, is known as gestational hypertension or induced by pregnancy. Often, high blood pressure in pregnancy is associated with urinary loss of protein (proteinuria) and, in this case it is called gestosi or preeclampsia. Precisely for this reason, blood pressure values are carefully checked at each obstetric check-up, during which urinalysis is always provided.
As the name suggests, hypertension in pregnancy disappears at the end of gestation. Of course, women who present one high blood pressure before pregnancy they tend to maintain their hypertensive state even during and after gestation. However, as anticipated in the introductory part, this magical event is accompanied by a physiological pressure drop, which requires a possible therapeutic adjustment or even the suspension of the same until the third trimester.
I greater risks occur when a previous hypertension is added to that induced by pregnancy, the causes of which are to be found inipoperfusione placentare, in reduced kidney function, as well as in the vasospasmo and in 'hemoconcentration.
One of the most serious clinical pictures associated with pregnancy hypertension is the so-called HELLP syndrome, acronym of the signs and symptoms that characterize it:
- Haemolysis;
- Elevated liver enzymes;
- Reduced values of platelets (Low Platelets).
In summary, thehypertension in pregnancy can be present in four distinct forms:
- Chronic pre-existing hypertension
- Gestational hypertension
- Preeclampsia/eclampsia
- Chronic hypertension + preeclampsia
Risks of Hypertension in Pregnancy
Hypertension occurs in about the 6-8% of all pregnancies and contributes significantly tostunting of the fetus, as well as fetal and neonatal morbidity and mortality.
In Western societies, in particular, hypertension in pregnancy represents the second cause of maternal death after thromboembolism, accounting for approximately 15% of all causes of death in pregnancy. The pregnant hypertensive is, in fact, more predisposed to some potentially lethal complications, such as:
- The detachment of the placenta;
- Disseminated intravascular coagulation;
- Cerebral hemorrhage;
- Hepatic and renal insufficiency.
Treatment and Prevention of High Blood Pressure in Pregnancy
See also: Medicines for the Treatment of Gestational Hypertension
The picture that emerged from the previous paragraph is rather disturbing; however, talk about increased risk does not necessarily mean talking about high probability. In fact, hypertension in pregnancy can be controlled through appropriate pharmacological therapies; however, it is essential discover and treat disorder at an early age, putting in place a whole series of preventive measures.
The therapeutic choice differs in relation to the type of pregnancy hypertension and its severity. When the condition is chronic, then pre-existing:
- In case of diastolic pressure compress between 90 and 99 mmHg the treatment is essentially behavioral, therefore aimed at the control or eventual reduction of body weight, the moderation of dietary sodium, and the abstention from alcohol, smoking and severe exertion. The risks for mother and fetus are quite low.
- If the pressure diastolic reaches and supera i 100 mmHg, the treatment is pharmacological and based on the use of drugs such as alpha-methyldopa, nifedipine, clonidine or labetalol. Also in this case, the risks for mother and fetus are low, but increase as the extent of the hypertensive phenomenon increases.
PLEASE NOTE: in the mild forms, the physiological pressure drop that occurs during the first trimesters of pregnancy often gives the possibility to reduce - and sometimes suspend - the antihypertensive drugs, which will then eventually be resumed in the last two or three months of gestation.
Some drugs used to treat hypertension are contraindicated in pregnancy; therefore, women of childbearing age suffering from chronic hypertension should consider the dangers associated with the use of ACE inhibitors, diuretics and sartans (to be avoided if you are trying to get pregnant).
In presence of pre-eclampsia the treatment becomes more articulated, so much so that a careful control of the patient, if any hospitalization with bed rest and accurate monitoring of delivery times. This event must be taken seriously in the face of episodes of fetal distress or worsening maternal conditions. Neonatal complications are mostly linked to the need to anticipate delivery at a very early stage, in order to limit maternal complications.
The National High Blood Pressure Education Program recommends starting the antipertensive therapy when the minimum pressure is equal to or greater than 100-105 mmHg; the World Health Organization, on the other hand, recommends lowering blood pressure when it is around 170/110 mmHg, in order to protect the mother from the risk of stroke or eclampsia; finally, for other experts, the PAD should be kept between 90 and 100 mmHg.
Il magnesium sulfate is the treatment of choice for the prevention and treatment of eclampsia.
PLEASE NOTE: Women who suffered from high blood pressure during pregnancy are at a greater risk of becoming hypertensive again as they age. The positivity to this test, which in some respects could be considered screening, should therefore be understood as a warning to regularly check your blood pressure (even after the term of pregnancy), and to implement all those healthy behavioral habits necessary to contain the cardiovascular risk (achieving and maintaining a healthy weight, abstention from smoking and drugs, moderation of alcohol consumption, regular physical activity, optimal management of daily stress and balanced diet).